
The Lamp on Stress and Vision
- Jul 24, 2025
- 9 min read
Updated: Jul 25, 2025
The understanding of myopia(nearsightedness, i.e. blur in distance), hyperopia(farsightedness, more difficulty or even blur at near, simply put), eye focusing problems, strabismus (eye turn), depth perception difficulties and the more. One may even begin to include diseases of the eye such as Glaucoma or Macular Degeneration at some point.
It all begins with understanding the adaptative response: stress.
To understand stress, we must first begin to understand some history. I have always said, that the history of medicine is just as important as medicine itself. Maybe even more important at times. Dr. Elliot Forrest, late professor at State University of New York wrote concerning the history of theory of stress to summarized.

Claude Bernard, a French physician, physiologist, philosopher, and researcher, articulated the idea that a significant characteristic of a living creature is it’s ability to maintain an internal equilibrium amongst the external changes of the environment. Maintenance of this constant internal equilibrium was a key objective of all vital living things, and that disease can be boiled down to the breakdown of the body’s ability to maintain this equilibrium or “constancy.”

Building upon Claude Bernard’s base idea, C. Judson Herrick contributed to the idea of “biological regulation” around 1924. He stated that biological regulation was beyond merely adjusting to changes in temperature, pH, and what not, but more broadly represented the “continuous readjustment of the organism to the flux of surrounding conditions…”
In the same decade around 1929, a Harvard physiologist named Walter B. Cannon clarified this process of the “steady state” into what is now called “homeostasis” coming from the Greek “homoios” (similar) and “statis (position) meaning the ability to have the maintenance the same state of physiology. Cannon attributed homeostasis as the first process. The second process was described to be “fight or flight” response. The “fight or flight” was to represent the preparation for the final action, but not the final action itself, that is preparing to attack or retreat.

Hans Selye, a Hungarian-Canadian, physician, was the one responsible for putting “stress” as a term into the medical terminology. Prior to Selye, this was a term in physics referring to the interaction between a force and a resistance that counters the force. Stress would be the force that would deform, while “strain” is the resulting deformity. However, Selye used the term “stress” to as the response. English not being his first language, used the word “stress” to describe his theory and response, it became ubiquitous across multiple languages. When he eventually understood the proper word “strain” being the proper label, the term had stuck across languages.

I will point out, that the word “strain” was used by Dr. William Horatio Bates (to whom the healing cult of the “Bate’s Method”) is attributed. I will also point out that Bates was right, as in my first post, about some things. He of course, did not have well articulated physiological models like today. However, before those came along, the damage to his reputation and most of his ideas were lost to obscurity for the most part. He himself did not attributed his methodologies as “The Bates Method” but rather stated himself that anything that eliminated the “strain” would lead to the cure of imperfect vision however it manifests.
Selye described this stress (the response) as “the non-specific response of the body to any demand made upon it.” This non-specific response can be initiated by many different stimuli. Dr. Elliot Forrest pointed out that a more appropriate definition of the stress is “the non-specifically induced response of the body to any demand made upon it.”
Selye noticed that regardless of the disease (measles, arthritis, terminal cancer, the common cold etc.), they all had similar series of signs and symptoms like loss of appetite, loss of muscular strength, low ambition, weight loss and the more. He described a a syndrome of simply “just being sick.” Selye’s experiments included injecting his animal models with varying tissue extracts—whether they be bovine ovarian or other organs, or whether he exposed them to X-rays, cold, heat or forced exercises or even prolonged immobilization, the physiological effects were the same and characterized by enlargement of the adrenal cortex, gastric ulcers and atrophy in the thymic-lymphatic system (including the spleen). The idea that the stress response is non-specifically induced, regardless of the cause, the stimuli, and the intensity, is fundamental to Selye’s theory. Future researchers did disagree. John mason and Richard Lazarus believed that the stress response can vary, depending on whether the stressor has a psychological component or is purely physiological. They thought that Selye’s description of the stress response is mainly activated by emotional or psychological arousal and the difficulties in separating the physiochemical effects from the psychological pain reactions from the various stimuli.
The star of the stress response is Adaptation. Adaptative response to maintaine equilibrium, counteract the effects of the stressors and make sure they are limited to the smallest area possible to be enough (therapeutic dose) to deal with the situation. Selye’s General Adaptation Syndrome is called general because of the general effect upon the body despite the type of stressor: whether be metabolic in nature, physical threat, or social.

In short, the adaptative response has 3 stages. A) The Alarm Reaction. B) The Stage of Resistance. And C) The stage of Exhaustion.
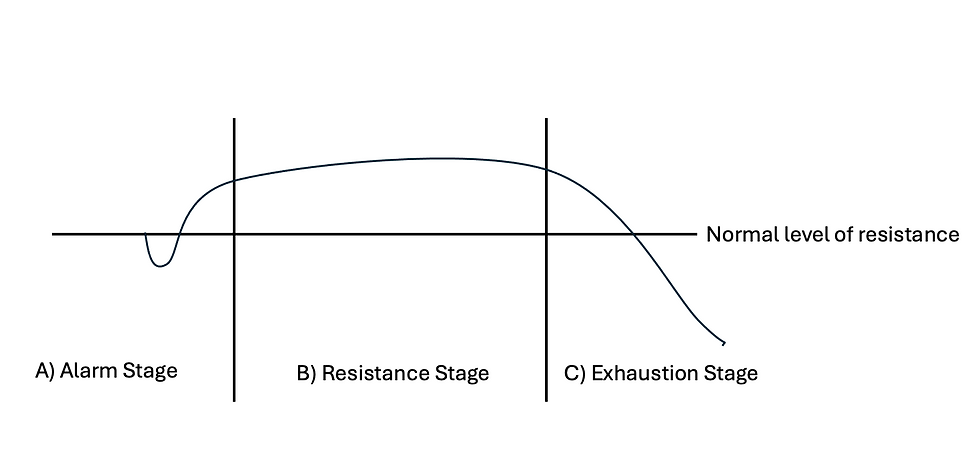
A) During the Alarm stage, activation of the sympathetic nervous system, enlargement of the adrenal cortices, discharge of adrenalin, lowering of resistance to the stressor, inhibition of the parasympathetic and more occurs. It begins in a “shock” phase lowering the resistance to the stressor and then the “countershock” phase during which resistance begins to increase towards its maximum and the defense mechanisms are initiated. It is necessary for the resistance to the stressor to decrease. Think in terms of physics. Momentum is mass times velocity. Velocity is distance divided by time with direction. Therefore, if you increase the time, you decrease the speed and therefore decrease the velocity. If then, the resistance to the stressor is lowered, the momentum that stressor has is also lowered. Modern cars are made to crumple more easily as to increase the time of impact vs impact with a hard steel shell will entail a higher momentum damage upon impact. Likewise, lowering of resistance to the stressor is a very necessary part for the survival at the shock stage as if the stressor is strong enough, could theoretically result in death. The alarm stage is metabolically expensive. Additionally, allowing the stressor to act upon the body, allows the body to accurately assess the action of the stressor and to mount the appropriate adaptative resistance response. Resistance must then activate to reign-in the alarm stage and begin adaptative resistance against the stressor.
B) Resistance state is basically the adaptation (explained later as four options) to the stressor. This is where resistance reaches its max and maintains that level of resistance until the body can react, localize and isolate the problem to minimize the stressor’s effect and restore normal functioning. Parasympathetic activation and therefore sympathetic inhibition begins. Adrenal cortices begin to acculmulate adrenalin. Resistance may then rise above the normal level. According to Selye, what truly happens during this time depends upon the direct effect of the stressor(s), the internal response to mount a defense, and finally the internal response to inhibit an excessive defense(which could then also become a stressor right?).
C) Exhaustion is the stage where all the “adaptative energy” is used up. Many times, some rest, redirection, change in environment, can restore the energy. This would be “adapative energy” at the superficial level. Think of this energy as money in a checking account. The other stage would be “deep adaptation energy” which would be likened to 401K, stocks, bonds or IRA funds. They are there, but accessible in finite amounts at quite a cost for access. When consistent and persistent exposure to perceived (key word) stressors exist, or simply too long-term of a stressor, a break down of the adaptive mechanism results, the Alarm stage is repeated, but now without adaptative energy stores, a condition then becomes irreversible… (or does it?)
It may indeed become reversible. I truly believe the answer is “It depends!” many times, one particular adaptative response breaks down and can no longer be utilized, but I conceive of “if there is a will, there is a way.” If there is a will to live, the body will find a way to maintain some level of homeostasis, even at a great cost to convenience. It may feel terrible, it may make you sick, but it beats the immediate alternative [death]. Hence, I have a model similar to described by Dr. Elliot Forrest and Selye: the multi-layers adaptative response. This is where different layers of adaptation are employed at different levels, some more extreme to relieve the earlier course of adaptative actions to free those resources up—hence chronic disease at the endocrine, structural change, or even immunological level. I would not have evolved my understanding without Dr. Forrest’s writings for sure, and they are built upon the established understandings of the neurological, endocrine system and neuroendocrine physiology.
What if since… being that Selye himself believed in a dymamic between eustress and distress. Selye believed that stress was an absolute necessity to life. To cease from stress was to cease from life itself and therefore death. The homeostatic mechanism needs constant engagement. I think of the adaptative series as a constant live-stream show that must keep on going. It shall not cease. The question is, eustress or distress? If you are not growing, you are dying. An example of eustress is to think of weight lifting. Lifting weights would be a eustress to initiate an adaptative response towards growth while distress would be “overtraining” and take a long time for proper recovery. This is the basis of Mr. Olympian winner Mike Mentzer in his one hard set philosophy with long recovery times to avoid overtraining. Keep the trainer in eustress and out of distress. Prolonged distress will lead to the exhaustion stage eventually if lasting long enough. However, what if eustress can be applied in a way to re-engage the adaptative system in a disease that has had multiple layers of adaptation? One will need the right stimulus and the right course of action. Physical Therapists engage this process all the time.
As written above, adaptation can be implemented in a eustress way to “peel back” the layers of adaptative response in many cases. That is just my personal belief. The question is properly identifying those layers, something that modern medicine and even optometry fails to do simply because they are aware that they should be identifying the layers of adaptation to stress. For example, myopia is a refractive error. It is an adaptative response. It would not otherwise exist. Much science has been done to show measures that can be effective in its slowing down or prevention such as sunlight, whole grains, liver, lack of stress etc. The question is, eye care professionals would think (had they be looking for an adaptive layer specifically) that the adaptation is an inherent structure change of the sclera. However, the first adaptative stage is simply neurological rewiring. What if then, myopia is a neurological muscular tonal change induce by the subcortical areas of the brain such as the cerebellum, basal ganglion layer or some other area. This would then confirm Dr. Bate’s suspicion on “the strain” as the cause of myopia and other disorders of the vision. Myopia could then be reversed, but one has to approach myopia with the multi-layered adaptative response model in mind.
The type of adaptation (occuring in the Resistance Stage B) that is employed depends upon the route. Dr. Elliot Forrest offers these as reasonable options:
1) Catatoxic (fight)
2) Syntoxic (flow)
3) Flight
4) Fright
Catatoxic: would be do to what is necessary to deal with the problem, whether be competitiveness, aggression, combat. Fighting the enemy so to speak. Hunker down and do what has to get done.
Syntoxic: if you can’t beat them, join them. Tolerate the enemy and reach equilibrium. This option revolves around living at peace.
Flight: avoid the problem instead of fighting or making peace. Procrastinate. Avoid the problem.
Fright: is basically an extreme version of flight towards the inward direction.
Each of these adaptative strategies have positives and negatives. If the General Adaptative Series loop is working repetitively, then the body could theoretically switch strategies if one is not working. They can be used to preserve or refill the “adaptative energy” hypothesized by Selye thus keeping the loop going.
I am of the opinion that ALL diseases and disorders, from myopia to Glaucoma to diabetes, should be viewed with the General Adaptative Model in mind. Because the effects of the stress response are non-specific and general. The autonomic nervous system (sympathetic and parasympathetic) does not do well to pat the head and rub the belly at the same time. The ANS has many things to do, so deeper layers can be employed as to free up the ANS. I will not elaborate further for the sake of time.
For the good news! Since the stress response is general and non-specific, one can use the vision to determine what the stage the individual is undergoing at the moment. What behavior is being employed. Is it an Alarm stage with poor resistance? Is there a prolonged resistance stage? What about exhaustion? How much resistance can be mounted before exhaustion occurs? All these questions and observations are, in my opinion as a behavioral optometrist, the core of behavioral optometry, founded in the established science of physiology. All the optometrist has to do is understand and Just Look! into the retinoscope and see how the person responds to a stressor. Every test I do involves this model, and it is very powerful in diagnosing and rehabbing the visual problem.
The eyes are truly the light of the body both spiritually and physically (words of Jesus Christ in Matthew 6:22), and therefore can be used as a lamp to understand what response the body is undergoing. What you can understand, you can then see. This is the LampSight.
Dr. Greg Johnson
Follow me on:

